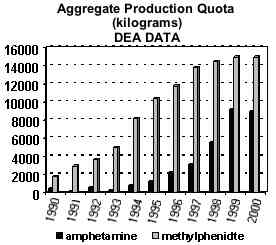
Amphetamines are essentially low-dose cocaine-class medications for increasing neurotransmitters in the brain. They invigorate the thinking-control pre-frontal cortex and so are effective for controlling behavior and attention in the short term. But they are palliative, treating symptoms not cause.
Many who don't like this plethora of medication claim that the ADHD problem must stem from:
over-diagnosis,
inept parenting,
teachers wanting easy classrooms,
the ability of pharmaceuticals to market products, or
pharmaceutical and food industries funding and publicizing research favorable to profit.
This web site disagrees with the first three of these claims and agrees with the last, the placebo-free results of Feingold for BHA and BHT being a striking example of what did not receive funding or publicity. Mostly, the claim here is that there has been plenty of muddled thinking in research, a bit of naivety in congress and some unwillingness of all to consider lifestyle change.
Funding History and Related Issues
Feingold's food and diet findings in 1973 were clearly a national concern. At least Sen. J. Glen Beall Jr. (D-MD) felt so. He entered materials into the Congressional Record, contacted the FDA and NIMH and sent a letter to Sen. Ted Kennedy (D-MA) asking that his Health Subcommittee invite Feingold to present findings in its next month's hearings on drugs.
The Senate hearing alleged in NutritionFoundation1980 and Wender1986 never happened. The LA Times wrote about a Ted Kennedy effort, but there is nothing in the Congressional Record to indicate any official action or public comment by him on the Feingold issue. Funding from government agencies did happen, though, and that was perhaps more logical than a Senate hearing. The issue was more technical than political. Could Feingold's observations be confirmed by others, and unlike clinical observations, in the way long established for avoiding subjectivity?
The NIMH Psychopharmacology Research Branch and NIE funded Conners, and the DHEW and University of Wisconsin funded Harley. True, psychopharmacology means medication by definition, which sounds like the fox guarding the henhouse, but the Psychopharmacology Branch could also be argued to be a logical agency for overseeing investigation of Feingold's diet-control observations. It had the experience of handling hundreds of cases of objective treatment trials.
Swanson received government funding in Canada for the work reported in the 1980 conference. Also Canadian funded, Triets did RAST blood testing to rule out food allergies.
The journal publications by Levy, Mattes, Swanson, Weiss and Williams cite no funding source, but it was probably industry's Nutrition Foundation because the works by these groups are summarized in NutritionFoundation1980, and there is some slight discussion of industry funding in the 1975 introduction. Also in the written record is that US government-funded Conners and Harley allowed their results to be summarized by the Nutrition Foundation and that Conners accepted money from the Nutrition Foundation and allowed them to do compilation of his data.
It is here where the possibility has to be considered that
industry
may have funded its choice of anti-Feingold professionals to sway technical results in the usual chicanery now so often seen. But that was well before the tobacco or global warming wars, and society was not yet suspicious.
Also known long before 1980 but not acknowledged in NutritionFoundation1980 or in Conner's journal reports were two unfortunate timing facts that cloud his works. The group was well into an open diet-control study when Feingold's book came out in 1974. So that first approach had to be abandoned and a closed (RCT) placebo-controlled double-blind protocol adopted. Beatrice Trum Hunter's suggestion that BHT and BHA should be removed from diets was not implemented and published by Feingold until the end of 1977, three years after his book and long after the Conners group was well into execution of their second protocol. They were hampered technically by being first, and too early. Their fist publication reports guarded conformation of the Feingold diet. Compare Conners1976 and the Conners section of NutritionFoundation1980.
Then too, hyperactive reaction times, according to Feingold and the FAUS support group, commonly last for three days and sometimes longer. But Harley1978a appears to be the main paper of the era that describes a procedure for tracking diet infraction rate and reports an actual number. In a letter to a Feingold parent he gave an infraction rate of once or twice a week. (Brenner1977) His final published rates on p. 821 are, depending on the age group, averages of 10.5 or 5.3 days between infractions. The other six research groups are less clear about or do not report infraction rates, and one can only wonder how often infractions repeated before there was time for ongoing reaction to wear off. Though referred, the medical journals all accepted these papers with their infraction rate-reporting omission, and none of the summary papers that followed noticed the problem, either.
In general, though, the papers show an evolution of awareness as to the details and care of what the diet is and the need to control infractions. Swanson1980 placed patients in a hospital to control the diet regimen. Weiss used patients enrolled in the Kaiser-Permanente Health Maintenance Organization associated with Feingold and excluded the BHA and BHT preservatives. Mattes1981 used practicing Feingold families. In spite of problems (Swanson1980 misunderstood the effect of recent medications. Weiss misunderstood salicylate and caramel as mentioned. Mattes1981 relied on the usual questionable challenges), there was a slight trend in these later papers reporting more correlation between diet control, challenges and behavior.
And it appears possible that quality of research might have been hindered by shortage of money. As pointed out, many of the papers cite no sponsor, but one can extrapolate from the funding discussion in the Nutrition Foundation's 1975 report. The average grant award to Levy, Mattes, Swanson, Weiss and Williams was apparently something less than $250K in equivalent 2010 dollars - not much before institutional overhead for trying to implement tight diet control for a meaningful number of patients.
Basis of Today's Dominant Medical View
Feingold was able to turn the symptoms of ADHD off and on repeatedly by eliminating or allowing food additives. He felt this was sufficient to prove his hypothesis, and in fact, the first thing other researchers did was to successfully repeat this type of "open" crossover A-B-A-B- type of study.(Conners1980Book, pp.12 + 16-19)
What the other researchers did not do, though, was establish that they could in fact implement Feignold's regimen by actually replicating his results - an open diet control with response rate of 30-50% before 1977 and 60-70% after 1977. And they never used Feingold as a consultant. So they were testing their version of Feingold's procedure, not his procedure. And they showed no hint of realization that probability of success with diet controls has more to do personality characteristics of the mother than with the patient ADHD child. This and a few obvious diet implementation mistakes were never noticed during the peer-review publication process. But as mentioned above, when the starting point procedures were tightened in Rowe1994, the results were different.
However, as vividly expressed in pages 16-19 of Conners1980Book, the accepted approach for establishing truth in medicine is by means of the Nobel-winning RCT or what is now called "closed" double-blind placebo-controlled trials of patient behavior. That is what received the emphasis. If it is placebo controlled, it is good research. There were seven research groups in all that did this type of study during the 1974-1981 time period, and their fourteen peer-review journal articles are gathered here in the section of the Paradigm Library titled "closed" as:
| peer-review journal reports | |
| of "closed" studies | |
| Conners1976 | |
| Goyette1978 | |
| Harley1978a | |
| Harley1978b | |
| Levy1978a | |
| Levy1978b | |
| Mattes1978 | |
| Swanson1978 | |
| Williams1978 | |
| Tryphonas1979 | |
| Conners1980 | |
| Swanson1980 | |
| Weiss1980 | |
| Mattes1981 | |
| journal summaries: | |
| Mattes1983 | |
| Wender1986 | |
| non-journal: | |
| NutritionFoundation1980 | |
| Conference1980 | |
| Conners1980Book | |
Tryphonas1979 investigated allergies and Williams1978 investigated medications versus diet, confirming medications more potent, so there were effectively six research groups and twelve papers that examined efficacy of controlled diet per se. Their protocols evolved with time. There were also eight clinical or "open" studies by: Brenner, Cook, Feingold, Palmer, Rapp, Salzman and Trites. Noone has ever recognized Feingold's results for preservatives as being independent of placebo.
For an introduction one could skim: AACAP1997, Mattes1983 (last section) and Wender1986 (Table 3) versus Rimland1983 and Rowe1994 (introduction).
Wender1986 is particularly well written and perhaps the main sustaining summary that, for decades, has locked in the way of thinking for all main-stream medical researchers. Mattes1983 is also an informative era review, but offers perhaps more interpretation than Wender1986 and seems interestingly different in tone than that of the previous two papers co-authored with Gittleman-Klein.
The Winder1986 review does not include Mattes1987, Swanson1978 or Mattes1981. But Weiss1980 and Mattes1981 are assessed here as the two best of the closed protocol studies of the era.
The outcome tended to be that the open studies found correlation between diets and ADHD but the closed placebo-controlled studies found almost none. The statistically insignificant exceptions to the latter were: 1) Conners1976 was tentatively favorable. 2) Harley1978 found that some preschoolers reacted. 3) Swanson1980 also found diet sometimes helpful for a few young children under the age of five, but increasing the coloring dose level to 100 mg induced reaction in 17 of 22 children. 4) Weiss1980, out of 22 children, found a mild reactor and a dramatic reactor. 5) Mattes1981 is discussed below.
Some researchers have pointed out the distinction that not being able to establish a link between diet and ADHD is a null result and not the same as a negative result showing no link exists. The latter, though, has been the widely accepted mainstream point of view.
Cookie Crumble
In 2010 the EU began requiring ADHD warning labels for artificial dyes. This was based on 2004 and 2007 University of Southampton studies by Stevenson et al. China followed in 2012, but not the US. FDA convened its 2011 Advisory Committee Meeting which, as pointed out, resulted in no action.
The EU labeling requirement is that foods containing certain dyes have to state that they "may have an adverse effect on activity and attention in children." This is not a regulation of the product, only a labeling requirement and does not apply to adult consumables like alcoholic beverages, but it was not supported by the European Food Safety Authority, counterpart of the US FDA, and it .
There are six dyes listed in the EU regulation, three of them allowed in foods in the US: Red 40, Yellow 5 and Yellow 6. (The regulations in China have not yet been translated. -- The nine FD&C certified colorings for use in foods in the US are: Red 40, Yellow 5 and Yellow 6, Blue 1, Blue 2, Green 3, Red 3, Orange B and Red 2. The latter two are for specific use, only. Water insoluble lake versions of the others except Red 3 are certified for drug use. Certification means that each manufactured batch must be confirmed by FDA testing to be chemically pure. FD&C is an acronym for the Federal Food, Drug, and Cosmetic Act of 1938. It established the FDA and was enacted following the Elixir Sulfanilamide disaster of 1937.)
In the US the only official change as of 2011 seemed to have been at the Mayo Clinic whose web site began to associate food dyes and behavior. Response from the American Academy of Pediatrics remained guarded (Corporate associations of these authors are respectively, 8 food, 2 pharm, 23 pharms, 1 pharm, a color-flavor + 7 food-beverage), with no response from the American Psychiatric Association, NIMH or other lead research organizations in the US.
The AAP's position began to change in July of 2018 with publications calling for strengthening of the Federal Food, Drug, and Cosmetic Act because of "endocrine and other adverse health effects" from food additives and calling artificial food colors, nitrates, and nitrites "additional compounds of concern". Any clear link to ADHD, though, is still specifically dismissed with the statement, "Data about health effects of food additives on infants and children are limited or missing."
By 2018 one would expect epidemiological studies to be coming out for the society-wide experiment underway in the EU since 2011. It's a wonderful opportunity for epidemiological study of a large population. Since the EU food labeling change, have incidence rates gone down for things like expelled from play school because not potty trained, late bed wetting, frequent self-destructive accidents, persistent immediacy, inability to learn from mistakes, insomnia, impulsive behavior of the young or criminal impulsivity in general, nasal polyps, ADD/ADHD, Asperger syndrome, ticks, obsessive-compulsive behavior, depression, teen drug use and teen/college suicides (while many of these have been going up in the US)? But there seems to be no such systematic, large-scale study or even interest in one. Lead author of the Southampton studies, Stevenson, says the EU has moved on, and in the US there seem to be no taste for following.
(It is perhaps worth noting that there are other examples of similarly long periods during which accepted understanding and perception has had to confront confusing observable evidence.
Stomach ulcers are now know to usually be caused by bacteria in the stomach, but that was hard to believe at first because stomach acidity is suppose to kill all microflora. The idea languished for 100 years after a pathologist first found bacteria in the stomach. It took a second pathologist to press the case, dramatically by first infecting and then curing himself.
The special theory of relativity and quantum mechanics now depict light as having a wave nature independent of any medium, but the absence of propagation medium was at first very hard to conceive. It was 40 years from the first apparently nonsensical measurement for the speed of light by Michelson & Morley to the development of the special theory of relativity.)
|
The APS DSM
(This section first written in 2012 and then revised in July of 2018.)
In its Diagnostic and Statistical Manual, the American Psychiatric Association has taken on the daunting task of listing definitive diagnostic criteria for all psychiatric ailments. DSM-V was in draft in 2012 with much debate and was revised in 2018.
This reviewer submitted a proposal both times that the DSM-V should find some way to acknowledge that most of the rest of the world thinks there is a link between at least some food additives and ADHD and that as of 2018 the AAP is specific that artificial food colors, nitrates and nitrites seem to be problems. The APS committee rejected the propsal both times (Drs. David J Kupfer, Darrel Alvin Regier, David Shaffer, Francisco Xavier Castellanos).
The DSM also fails to mention one of the rather consistent and obvious symptoms of ADHD, late bed wetting and being expelled from kinder garden for not being potty trained. And some of the so-called comorbid conditions should probably be reclassified as due to the same cerebral enzyme imbalance as ADHD. Here's an example maybe involving both the prefrontal cortex and the pleasure center shell of the nucleus accumbens.
1 - This is of a little girl who the parents described as easy and charming but sometimes prone to outbursts in relation to chocolate or bubble gum. They reported a note from preschool recommending they take her to an occupational therapist because of multiple behaviors showing "need for self stimulation" -
 things like holding her head upside down, bumping others and talking out of turn not related to her environment. And this observer noticed that she would sometimes sit on the ground spread eagle playing quietly with a baby doll in one hand and massaging her crotch with the other. Here she is
(Hold cursor over lower part of rectangle.)
in an on-stage dance-school performance with six other aspiring tutu-dress ballerinas about age four. None of the others self-stimulate the way she does. Is this need due to artificial food ingredients? The model suggested here is that lack of dopamine is not just to the prefrontal cortex but also to the pleasure/reward center as well. The problem needs to be figured out before the little girl becomes a teenager. [Update 14 yr later: He became a trans.]
things like holding her head upside down, bumping others and talking out of turn not related to her environment. And this observer noticed that she would sometimes sit on the ground spread eagle playing quietly with a baby doll in one hand and massaging her crotch with the other. Here she is
(Hold cursor over lower part of rectangle.)
in an on-stage dance-school performance with six other aspiring tutu-dress ballerinas about age four. None of the others self-stimulate the way she does. Is this need due to artificial food ingredients? The model suggested here is that lack of dopamine is not just to the prefrontal cortex but also to the pleasure/reward center as well. The problem needs to be figured out before the little girl becomes a teenager. [Update 14 yr later: He became a trans.]
The point is that ADD is often observed simultaneously with emotional conditions like need for stimulation or drugs, thrill seeking, mood swings or depression and rage control problems or criminality. And as described below, it is not unreasonable to suspect that ingesting foods containing metabolic-waste-product-like compounds might overload PST, compensation then initiating elevated MAO and thereby reduction of monoamines like dopamine in the brain. The APS doesn't have a clue even enough to disagree.
2 - The second example somewhat related is of a 34 year old women who this observer met about 8:30 in the evening, on Christmas eve, by the side of the road, holding out a cup. She was in a wheel chair with affixed tray top and not near enough to passing traffic to be as noticeable as most pan handlers. Her problem was multiple sclerosis, and with it, depressed mood. She was hungry for conversation, but often had to write out a word or phrase when her slurred diction was unintelligible. She had joined the Army after high school but was given a medical discharge a few years later and became a ward of the state. What she wanted most after fifteen years of steady MS degradation was to "meet her maker," and she used that phrase several times in less than an hour.
She did not display suicidal ideation, indecisiveness or fatigue, and did not appear to fulfill the DSM definition of "major depressive episode," but was being given Valium and occasionally Prozac. (The location: Fletcher Ave crossing under I 295 north of Tampa. The year: 1981 during the depth of the Reagan-Volcker recession. Her name: Pat Clark. Her clinic physician: Dr. Kailie Shaw at the Psychiatric Center, University of South Florida in Tampa (813-974-8900, 3515 E Fletcher Ave, Tampa, FL 33613).
Here is some of her medical history as probed during that conversation and recorded in this observer's written notes. There was never any hesitation in her response when asked about an event or her age when it occurred.
| Age | Symptom |
| 13-14 | First vaginal yeast infection, reoccurrence thereafter about once a year. Urine turns green. |
| 15 | Allergic to penicillin (intestinal cramps and constipation for a week) |
| 16 | Gas, diarrhea |
| 16 | Two months of flakey lips |
| 17 | Cancer of the cervix |
| 19 | Severe MS with coma for 10 months |
| 21 | Fuzz growth begins under toenails |
| | persistent reoccurrence of oral thrush and athletes foot |
This patient had never before been queried about Candidiases, was not being given Nystatin or other anti-fungal and was unfamiliar with the concepts of low carbohydrate diet or side effects from antibiotics. She was a heavy smoker, the methanol and in situ formaldehyde from that probably being a main cause of her MS. But one can't help but wonder if acetaldehyde from Candida was contributing as well.
Modes of damage from intestinal fungal overgrowth are apparently from production of acetaldehyde, malabsorption through the gut lining and leaky gut with mental effects from opiate peptides. These are generally unrecognized. The APS, for instance, does not include any concept that depression could be caused by Candidiases (or food additives, or trace methanol.) The methanol problem is even less recognized, including in the obviously partial combustion of tobacco.
Feingold Program Treatment of ADHD
The place to read about the Feingold diet -- what it is, how to do it, what is right about it and supporting research -- is Feingold.org. The recommendation is to start with a strict "Level 1" diet restricting artificial coloring, artificial flavoring, the petroleum-based preservatives, natural salicylate and several other problem foods added to the list since Feingold, including corn sweetener, caramel and bleached flower. Chocolate is allowed but recognized as the next most common food causing hyperactive reactions. And there is some argument for removing common allergens and even tyramine foods as well, to further reduce sulfa conjugation load. Ingram1997 v. Waring1997.
Many parents at CHAD meetings say that diet controls did not work for them, but a good many Feingold association parents and researchers find the opposite - that ADHD symptoms tend to disappear if foods with artificial chemicals and salicylate are avoided. That's for 70-75% of cases if "assiduously avoid" is pursued. And if food allergens are removed as well, the results apparently improve to 80-90%. So the current results are considerably improved compared to the 30-50% Feingold initially estimated, (and that the Nutrition Foundation reports as about the improvement achieved by quitting medications).
This high success rate of the Feingold diet is for ADD/ADHD only, and not for
autism
or Asperger's syndrome (a variant of autism free of linguistic and cognitive impairment).
The Feingold Program is occasionally dramatically effective for autism spectrum disorder, but generally no more effective than a gluten/casein free diet or other attempts to treat this perhaps related but more difficult ailment.
And it should be noted that the Feingold diet success statistics for treating ADHD are for controlled test environments. Every day families shopping in every day grocery stores can be expected to fail more often. A particularly useful aid for implementation is the FAUS "safe foods list" giving products by brand name.
The suggestion here is that probability of success of the Feingold diet depends primarily on characteristics of the mother and has little to do with severity of symptoms of the child ADHD patient. Fathers usually don't or can't contribute very much because they typically don't see or comprehend as well, and a good one at least doesn't resist. The required mother characteristics are: must be perceptive, must be determined and must have control of all the food environment at home, at school, with the father and preferably with the extended family as well. Success is not assured for split families. All foods, drinks, tooth paste and vitamins in the child's environment should be acceptable and everyone he or she sees should be eating the same thing. Putting only one child on a special diet is formula for errors and cheating, and one infraction every few days will render the diet ineffective. So will having been on medication recently. Seemingly unbelievably small minutia really do count. It is not true that "a little bit" is normal.
Treats usually involve sugar, and that is OK in spite of complaints like, "As a parent, the one thing I know for sure is to keep my kids away from sugar, particularly late at night. You give a kid sugar, and you're putting all the wallpaper at risk. One small Halloween-size bag of M&Ms and - boom! - they're running through the house, crayoning the walls, trying to put the cat in the microwave, beating the dining room table..." (Tony Kornheiser, The Washington Post, Feb 6, 1994, p. F1) The trick is to distinguish between "sugar" and "sugar products."

|
|
OK with Not OK Candy
|
Today's consumer interest in additive free products is affecting the marketplace and making it easier to follow the Feingold regimen. Some manufactures now market two versions of a product in almost identical looking packages, the original with additives and a newer version without. Distributers are responding as well, Whole Food's stating that, "We feature foods that are free of artificial preservatives, colors, flavors, sweeteners, and hydrogenated fats," and even more categorically Trader Joe's stating that its logo on products assures "no artificial flavors, colors or preservatives; no genetically modified ingredients; no MSG; and no added trans fats."
It's not quit clear whether these claims are entirely true, but buying at these stores does offer parents a low-effort approach that may be good enough to reasonably settle a mildly effected ADHD child or at least get some problem children through kindergarden. One does need to be careful not to pick up an additive-loaded instead of additive-free product when they look almost the same and are side-by-side on the grocery store shelf.
|
|
"100 % carrot juice"
|
|
contains unlisted lemon and water
|

|
|
"ALL NATURAL Lemonade"
|
|
doesn't taste like lemon
|
Reasons to doubt the accuracy of the blanket additives-free claims by Trader Joe's and Whole Food's are that:
1) Many of their products use "organic crystalized cane juice" and other deceptive wording tricks just like the rest of the industry.
2) The companies seem to be unaware of the BHT preservative used in the vitamin enrichment of milk.
3) The companies often do not respond to questionnaires for details of product ingredients.
4) Part of the latter problem may be that the companies do not recognize the authority-figure conflict that is unfolding concerning food additives. FAUS is the authority for food additives that cause ADHD, not the FDA, USDA or NIH. With decades of experience FAUS knows, for instance, the problem ingredients that are approved for omission from food labels, and when a banana blight in the tropics might be causing problems for some in the U.S. That is so unofficial that, of course, manufacturers and distributers have trouble with it.)
Flaws in the Formative Research of 1974-1981
(six subsections)
1) The Randomized Control Trial - Placebo Controlled and Double Blind
The Nobel award winning randomized control trial or RCT has been the gold standard in some half million medical investigations since the methodology was established in 1948 by statistician A.B. Hill while evaluating streptomycin for treatment of tuberculosis. Objectivity and reproducibility are reasonably assured in the hard sciences dealing only with instruments, and materials, but medicine deals with people and their subjectivities. The central achievement of the RCT is careful control to eliminate placebo. "Double blind" or "closed" testing means that testing is done both with a comparison of the real potion versus a disguised benign substitute and also with neither the patient nor the administrator knowing which is being administered.
And for the testing of whether diet controls can effect ADHD, two additional layers of procedural caution have to be added to prevent subjectivity from swaying results. The potions to be tested include colorings and flavorings, so if capsules are not used something has to be done to disguise these compounds in foods. Also, the unit of measure of effectiveness of the remedy is not inherently objective like a blood test. It is patient behavior that has to be evaluated, so tight procedures are required to make this as non-subjective as possible.
A third layer of added precaution that should probably have been added but was not is the mentioned need for some sort of control or at least metering of the "only a little bit" incredulity in patients and experimenters. The detail of the Feingold diet is for most not a priori believable.
Underlying all this is the fact that medical researchers must strive with all diligence not make any mistake of deciding something is true and worthy of promulgation to practitioners when in fact it is not. False positives are, in a sense, more important to avoid than a null result. The possibility of this kind of bias in the 1974-1981 studies of diet versus hyperactivity is not evident on first reading. In addition to patient placebo and evaluation subjectivity, they also attempted to achieve diet compliance.
But the diet was, unfortunately, somewhat still evolving in 1975 and misunderstandings were neither acknowledged at the time of publication nor in the summary papers that followed. They can be discerned, however, in the tightening of diet protocols with successive endeavors. Feingold was not included in any of the protocol designs, but after the initial studies, his criticism that the diet was not being strictly followed did lead to tightening of later protocols and eventually, in the last study of the period, use of Feingold Association families to administer the diet.
And more could have been done to minimize the likelihood of a null result. An introductory period could be used to see how well patient families can actually follow the diet. Or an introductory period in which the placebo food was used as a challenge, could be used to see if the placebo food was truly benign. Only the last study did the this, Mattes1981, with interesting results. And finally, but perhaps most important, tracking and reporting of diet infraction rate is needed.
The difference in tartrazine results for Rowe1994 and Levi1978 has been pointed out in the section on "Official Inconsistencies." Protocols for controlling placebo are similarly rigorous in these two papers, but not the control and assessment of diet. Rowe1994 started, for instance, by gauging diet success of participating families for a significant period of time before the trials started, but Levi1978 did not. Rowe1994 found a correlation between tartrazine and behavior. Levy1978 did not.
Six areas of research error are listed in the second line of links at the top of this page, and it is suggested that the placebo-controlled endeavors all erred in three to five of the following:
unrecognized protocol bias,
not fully understanding or implementing the said food controls,
not realizing the lasting effects of medication,
often failure to remove BHA and BHT,
use of salicylate in both challenge and placebo,
failure to monitor and report diet infractions,
no stated procedure for countering "only a little bit" incredulity of patient and researcher,
2) The Dose Issue
With the exception of Weiss1980, who used the faulty drink, and a few studies that used capsules, the placebo-controlled studies of the 1974-1981 time period all used the same specially prepared cookies for the challenge versus placebo. Section 2 of the 1980 Nutrition Foundation report states that:
1) capsules ruled out because the treatment to be evaluated is a food diet,
2) artificial flavorings would be impossible to disguise in foods,
3) "most of the chemicals contained in artificial food flavorings are identical to those that occur naturally in foods," and
4) Feingold had de-emphasized salicylates.
And, unfortunately, the artificial preservatives BHT and BHA were not yet known to be an issue, TBHQ not even existing, at the time challenge and placebo food protocols were being established. So the challenges were foods that:
a) contained artificial food colorings only,
b) used coloring dose level low enough not to cause noticeable stain,
(< 13 mg/cookie or < 36 mg/soft drink)
c) used chocolate to disguise the coloring, and
d) had no restriction on preservatives or salicylate.
Two cookies with a blend of nine colorings were designed to have a total amount more than half the US average daily consumption of colorings in 1973 and 1974.
(Amount of FT&C produced / # people in US = 27 mg/day and a study for children found 36 mg/day)
Much debate has followed about the dose level of the coloring, and it was not just diet proponents who doubted the sufficiency of the challenge cookies.
Mattes1981 p. 717 quotes a USDA survey that found 50-60 mg/day average intake of artificial food coloring for children in the US. Weiss1980, in their last paragraph, state that the Nutrition Foundation cookie challenge dose levels they and most other researchers used were about a fiftieth of the FDA allowable daily intake. The Mates1983 summary devotes two columns to the dose level issue.
The National Academy of Sciences estimated for 1977 that the average amount of food dyes actually consumed, was 327 mg per person per day.(p. 20, FAUS Bluebook)
And how much coloring is there in specific products like a packet of M&M's or a tablespoon of Ampicillin? Vendors are not required to tell, and won't, but one can experiment. The takes at least 150 mg of coloring to make the icing on one cupcake a nice shade of yellow.(Shula Edelkind, Dec 2010 FAUS Newsletter)
Swanson1980 was the only study to use challenge dose level commensurate with the higher than average amount of colorings that some people consume. This study used 100 mg and 150 mg dose levels because 150 mg had been assessed as the 90th percentile level of consumption in a memorandum between HEW and FDA. The memorandum was apparently not published in the open literature.
3) Challenge Food Errors?
Children have trouble taking pills, and it is impossible for the very young, but one has to wonder if some form of small encapsulation should have been used more often to disguise the challenge coloring. A few of the 1974-1981 studies did this, and they tend to be the ones that found more correlation between diet and behavior.(comment needs detailed expansion)
But, OK. Nutrition Foundation cookies were almost universally used. The challenge version with coloring and the placebo version without were indistinguishable. There are reasons to wonder, however, whether they were really diet-worthy.
In the last of the studies dated 1981, Mattes and Gittleman-Klein started with a one week trial of diet plus non-blind placebo cookies. Two of twelve children reacted to the placebo cookies. Mattes and Gittleman-Klein proceeded by eliminating those children from their controlled trials, but there is another interpretation. Their result could suggest that something was not quite right with the cookie formula. And the possibility has not pointed out in any review article, pier-review journal, society, agency or promulgation authority.
The ingredients of the standardized test and placebo cookies were not published in the open literature. FAUS recommends unbleached flour and finds problems with the unlisted preservative in milk, probably also a cookie ingredient. And though chocolate is allowed on the literal Feingold Program, chocolate, and especially dark chocolate, is known to be the next highest problem food for causing hyperactive reactions. (That's perhaps not surprising, because chocolate contains several methylated xanthines known to have sympathetic neurologic effects like dilation of airways and stimulation of heart rate.) The Weiss1980 protocol starts with the salicylate error mitigating challenge versus placebo drinks. Could there be a similar problem with the universally used cookie formula stated to have "natural ingredients"?
4) Journal Peer-Review Errors
Reports in research journals are supposed to be critiqued before publication by anonymous experts in the subject field, but this process for the 1974-1981 placebo-controlled studies may have been lax. Science magazine should not have published the Weiss1980 paper reporting use of a salicylate to disguise distinction between non-colored and colored drinks - or at least the authors should have been coached as a requirement for publication to qualify worth of the protocol. (Both the 2011 FDA Committee and Weiss in his answers to the Committee were still unaware.) And Pediatrics should not have published Williams1978, or at least not with the title and slant as submitted. Of course medication effects are more immediately noticeable both because they act directly on neurotransmitters and because ingestion of compounds causes an immediate change in body chemistry while metabolization of compounds is slow.
And several of the journals published reports that did not keep track of diet infractions and offer no hint of how often they occurred. (paragraph needs editing)
5) Experimenter Subjectivity
Even carefully designed randomized control trials become invalid if the people who design them have difficulty conceptualizing or accepting the exact details and minutia of the procedure to be tested. If there is any inclination to feel any part of the procedure is absurd and nonsensical, it would be best for test organizers to recuse themselves.
The Feingold diet is such a case where proponents make odd claims about a priori inconceivable minutia - so a step for minimizing the likelihood of null result could be to put those proponents in charge of implementing their regimen. The lead experimenter must control challenge testing, and both sides need to council and approve what the other is doing. The listing of Feingold as a member of the Expert Advisory Group in the Nutrition Foundation report, does not mean he was included in any protocol design or implementation. Rather, the mentions of Feingold in the literature are to his comments on studies already completed. And it was not until the last two studies in the 1974-1981 research period that Feingold Association families were used. Feingold Association leaders have never been used to implement a diet control testing protocol.
6) Detail Flaws
section needs revision especially of some statements that are too global - Conners1976 well done...
Attention to detail was attempted but often not very well in the 1974-1981 studies. There is no expression of realization that having taken Ritalin recently makes the diet ineffective, that salicylate should not be used in placebo test foods, or that a violation in diet detail every few days can vitiate effectiveness of all other diet controls. Rimland1983 points out the latter but has been ignored. And in recent decades FAUS has updated its safe foods list of brand names every year. Vendors change product ingredients, making the Feingold diet somewhat of a moving target, but this level of detail is not mentioned either in any of the 1974-1981 studies or in later reviews.
With the exception of Weiss1980 and Mattes1981, the research groups all relied either on average families to follow instructed diets, or (Williams1987) used hospitalization to control patients who were taken off Ritalin for the duration of the testing. And, as mentioned, none of the research teams ever used leading diet proponents to council or handle the patient food controls. The Weiss1980 and Mattes1981 protocols were better and a period-end culmination for diet implementation during testing. They used children already on the Feingold diet for whom parents reported marked behavioral benefit with marked deterioration when given artificial colorings. The researchers limiting themselves to challenge testing and evaluation. Weiss1980 explicitly mentions excluding BHA and BHT preservative from the diet. Mattes1981 does not. (BTHQ did not yet exist.) But Weiss1980 also mistakenly used salicylate, a diet violation, to disguise both food challenges and food placebos. None of these protocol errors have ever been noticed by NIH, AACAP, lead mainstream researchers, the Nutrition Foundation or now the 2011 FDA Advisory Committee.
One of the more carefully executed studies during the formative 1974-81 era was Mattes1981 with Gittleman-Klein. They used Nutrition Foundation cookies with one week duration periods for challenge versus placebo testing. A week schedule started with one cookie on the first day and ramped to six on days six and seven - an escalation from 13 to 78 mg/day if they were challenge cookies. They found no correlation between colorings and hyperactivity or distractibility.
They note several qualifiers in their work. Two children were eliminated before the trials because they reacted to the placebo cookies. Eleven children were tested. The actual diets used were not analyzed or monitored. Five of the children tested were demonstrating ongoing hyperactivity behavior independent of challenge testing and in spite of the diet. Only three children could be diagnosed retroactively as cases of hyperactivity. And challenge coloring dose level was 1/50th of the maximum allowed daily intake recommended by the FDA, those levels having a 100-fold margin of safety as extrapolated from toxicity testing in rodents. (They do not mention BHA, BHT or salicylates.)
ADHD Models
There are two classes of modeling to explain how ADHD occurs, the dominant majority medical view and the opposing less known medical view. Both sides agree that there is a heredity factor in at least 50% of cases, and both sides agree that suppressed prefrontal cortex can directly cause attention deficit and indirectly cause hyperactivity because of subnormal judgement control over impulsive responses from the subjective limbic system. Ritalin and other amphetamines are low-dose, cocaine-class stimulants that reduces hyperactivity by reinvigorating the prefrontal cortex. The disagreement is over how the prefrontal cortex becomes suppressed.
1) The dominant majority view is that ADHD is an innate biological condition - a hereditary hard-wired brain anomaly. PET scans have shown sub-normal glucose metabolism in regions of the prefrontal cortex with further deactivation of the right frontal lobe and the anterior cingulate in response to attempts by the ADHD patient to perform concentration tasks, but reproduction of these results is problematic. MRI imagery shows slight reduction of structural sizes in the right frontal lobe, the anterior cingulate, the Caudate nucleus, globus pallidus and the cerebellum. And correspondence has been found to specific genetic alleles of the dopamine D4 and transporter genes. This leads to the conclusion that ADHD is a physical brain anomaly with no environmental causal factor and that comorbid conditions such as ticks, depression and mild schizophrenia are distinct, separate problems. Russel Barkley offered what some call a unified theory of ADHD: "...impairment in response inhibition... of the orbital frontal cortex and subsequent connections to the limbic system... but the neural underpinning of ADHD has yet to be elucidated."
The brain structure size statistics reflect differences only between groups though, and are not sufficient for diagnostics, the variation within a normal or within an ADHD group being larger than the variation between the groups. Data analysis in the most exhaustive study involves adjustment of means by a factor of 14 times standard deviations, and it is only then that normal and ADHD groups are found to have statistically meaningful differences in size of brain structures. This ten-year study is apparently the culmination of a mid 90's decision in the Child Psychology Branch at NIH to allocate its resources to the use of anatomical MRI. There is no conclusion about how differences in size of brain structures, or most surprisingly the cerebellum, could cause ADHD.
[See CastellanosVideo,
Castellanos2002/info, APA2010BrainStruct/info and Ivanov2010/info.]
(Behavior modification training is sometimes also called "brain exercise training," with the claim that it expands deficiently small regions of the brain - tocureadhd.com)
2) A tentative alternative model from some in the opposing community suggests that ADHD is due to enzyme problems rather than anatomy. The model is referred to here as the Ingram-Sinaiko PST deficiency model. PST (phenol sulfotransferase) is one of the enzymes that cleans up waste phenolic and sulphate products from the body's normal chemical pathways, and in some people the production of PST is deficient. There may be just enough PST to satisfy normal body functions until artificial chemicals that mimic normal waste products are added by ingesting them orally, at which point the supply of PST clean up enzyme becomes insufficient to handle the additional load. In the brain this clean up insufficiency must be overcome, especially for removing tyramine, and the deficiency is compensated by increased production of MAO (monoamine oxidase) - an enzyme whose primary clean up function is to reduces longevity of five critical neurotransmitters (dopamine, epinephrine, norepinephrine, serotonin and histamine).
Ingram1997,
Sinaiko1996,
IntroPST,
PST
 By this model one would expect not only suppression of the prefrontal cortex and hence ADD/ ADHD, but also suppression of other parts of the brain and so other symptoms as well. All drugs of addiction target the shell of the nucleus accumbens, and low dopamine to this pleasure center could reasonably be associated with depression or need for satiation as in drug use, thrill seeking, risk taking and excessive sexual behavior - all common with ADHD. Violent behavior, depression and obsessive-compulsive disorder are known to be associated with low levels of serotonin.
By this model one would expect not only suppression of the prefrontal cortex and hence ADD/ ADHD, but also suppression of other parts of the brain and so other symptoms as well. All drugs of addiction target the shell of the nucleus accumbens, and low dopamine to this pleasure center could reasonably be associated with depression or need for satiation as in drug use, thrill seeking, risk taking and excessive sexual behavior - all common with ADHD. Violent behavior, depression and obsessive-compulsive disorder are known to be associated with low levels of serotonin.
This unified mechanism for diverse and possibly simultaneous cerebral dysfunctions makes the standard emphasis on precision diagnostics to distinguish between ADHD and comorbid symptoms seem to be a misdirection. The now common depression in children is as dramatic as the 90's jump in incidence of ADHD, and the two phenomena may be related rather than distinct. And in this view it is inconsistent to administer antidepressants for OCD to raise serotonin and then also use Tic Tacs for reward motivation with "Virtual Camping" therapy.
The enzyme PST-deficiency model has not been confirmed, however, and it is incomplete even in principle because the chemicals recommended for diet avoidance for controlling ADHD are not all phenolics. And there is no explanation for differences in reactivity such as which coloring causes the stronger reaction or why some are acutely responsive to the cited class of salicylates while many are not. (And OCD, though related to low serotonin, is now identified by PET as related to over-activity of the orbitofrontal cortex and caudate nucleus. It is a case where "midfulness" training does work. Schwartz J, Discover Magazine, Nov 2013, p.55.)
Candida albicans, 1980
So how can enzyme deficiency occur? One answer may be intestinal overgrowth of yeast or other fungi resulting from the modern triple assault of oral antibiotics, high-carbohydrate diets and exposure to wide range of chemical compounds. These three factors all tilt the normal balance of friendly bacterial microflora growing in the gut to potentially damaging yeast. Intestinal overgrowth of unfriendly yeasts is commonly referred to as Candida, leader of the pack. Dysfunctions can include intestinal and mental problems as well as the immune, hormonal and metabolic systems probably relating to or adding to ADHD.
Candida does not cause disease in the usual sense but more a change in general health or state of being, potentially devastating. Treatment for Candida is aimed at achieving normal microbial balance and can not remove all of the pathogen. And there is conflict with the administration of antibiotics so useful in treatment of disease.
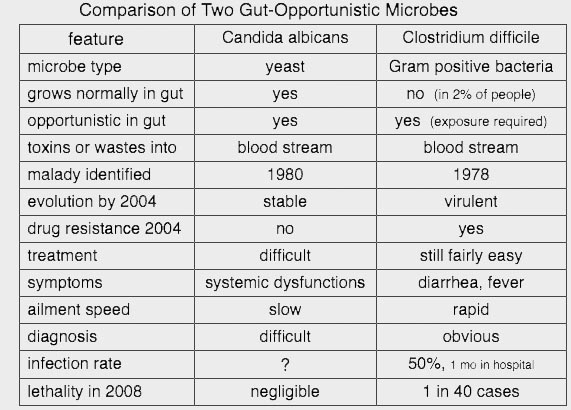 One way to describe Candida albicans is by noting its similarities and differences compared to better known Clostridium difficile. Both become likely following use of antibiotics. C. diff is recognized and treated because it inflicts obvious symptoms, rapidly becomes serious, is potentially fatal and in 2008 suddenly jumped to become recognized as the second-ranking hospital scourge infection.
One way to describe Candida albicans is by noting its similarities and differences compared to better known Clostridium difficile. Both become likely following use of antibiotics. C. diff is recognized and treated because it inflicts obvious symptoms, rapidly becomes serious, is potentially fatal and in 2008 suddenly jumped to become recognized as the second-ranking hospital scourge infection.
Candida, on the other hand, poses little threat of fatality, has no reliable lab test diagnostic, is slow to inflict symptoms, and when it does, causes mostly indirect system dysfunctions that range in diversity too broad for some like the AAAAI to believe. This wide range of disparate reactions has been discovered, however, three times by totally independent groups - first in the 1940's through 1970's by Clinical Ecologists, then in the 1980's by Candida proponents, and finally again in the 1990's with Feingold Program refinement and extension by FAUS.
(It should perhaps also be pointed out that, like Candida overgrowth and though many of the symptoms are different, the symptoms of low but persistent carbon monoxide poisoning are also diverse physically and mentally and can also pass as unrecognized or be misdiagnosed. In principle CO poisoning is well understood and clearly diagnosable with a $40 blood test. But the blood test is not standard medical practice and some 34 million people in the US live in HUD-approved trailers with intake vent only three feet from the furnace exhaust vent. A long list of diverse medical problems could have many causes, but may be more indicative of carbon monoxide poisoning than Candida overgrowth for someone is living in a mobile home. See ABCNews2009.)
The initial idea for how intestinal Candida could cause systemic damage came from C. Orion Truss in 1980. Too much yeast growing in the gut can act as an internal pollution machine with acetaldehyde and other waste products and toxins pickling the body's chemical pathways. Vitamin B6 utilization is particularly important, for instance, because in various forms, it is the activator on half the body's enzymes. Enzyme loss can result in chemical sensitivities far wider in scope than classical allergies, and endocrine dysfunction implies a long list of some 26 possibilities including hypothyroidism, diabetes mellitus, pernicious anemia, spruce, celiac disease, lupus, rheumatoid arthritis and other autoimmune disorders. (Trowbridge&Morton, pp 325-329)
Then in the decade following Truss, other mechanisms for damage by fungal overgrowth were realized. Overgrowth of intestinal fungi may damage the intestinal mucus lining, likely effects being intestinal inflammation or Crohn's disease and also cause leaky gut syndrome - an increased permeability with passage of large molecules and partially digested foods including opiate peptides and perhaps oxalates into the blood stream.(ref1 v
ref2)
Even small quantities of food, opiate and oxalate molecules in the blood stream mean food allergies, mental problems like bipolar depression and tendency for kidney stones. (This opiate peptide mechanism for cause of depression is in addition to and before the above mentioned denial of dopamine to the brain's pleasure center.) And other abnormalities can occur if the acidity of food chyme leaving the stomach is not neutralized in the duodenum. Acidic Ph can degrade digestive enzymes in the gut, and in the brain, slow synaptic neurotransmitter activity starting about a half hour after eating. This panoply Pandora is often referred to simply as "Candida," the name of a leader of the pack of yeasts that rots flesh when we die and seems to like to get a head start if it can.
The Candida effect is more accepted in Britain than in the U.S. where mainstream medicine tends to treat vaginal yeast infection only and does not accept the possibility of systemic conditions from overgrowth of fungi. Here are three examples.
|
1) Infant ear infections are common, with insertion of tubes almost a norm to facilitate middle ear drainage. A pattern here is use of antibiotics to treat an immediate problem, this exacerbating an underlying problem of opportunistic Candida which in turn further damages the immune system making repeated use of antibiotics more likely - all without administration of antifungal medication, probiotics or low carbohydrate diet and often with no inquiry about standard allergens such as carpeting, pet dander or foods. (Some quantification of this trend is in a 2009 study that found reoccurrence of middle ear infection up to 3.5 years after treatment with antibiotics.) If the -PST+MAO enzyme model of is correct, this type of childhood revolving door antibiotics could be a leading cause of ADHD.
2) The higher incidence of urinary tract infection in women is considered to be caused by the anatomical fact that in women the urethra is closer to the anus. But proponents of Candida effects point out that multiple pregnancy, female hormones in general and an additional cavity inviting colonization all make women more vulnerable to Candida, so that treatment for fungi should be considered when there is a urinary tract infection. The antibiotics used for urinary tract infection are particularly strong. Using them with no antifungal medication may worsen the underlying condition - in a feedback loop similar to that just described for ear infections.
3) Another example is that in the treatment of depression, the possibility of leaky gut releasing peptides and opiates into the blood stream is never considered. This is shown in a Jan 2010 PBS video
that includes the case of a girl who slid into depression at puberty. There was no consideration of antifungal treatment and no inquiry into any possibility whether antibiotics or carbohydrate diet with female hormonal change might have stimulated growth of Candida. And when all anti-depressive medications failed, the treatment moved to last-resort
electroconvulsive shock therapy. The electroshock devices may be downgraded by the FDA to
"low risk."
|
Design of medications for attacking Candida is limited by the similarity in cell wall structures of yeasts and of cells in the human body. Non-systemic Nystatin and systemic Fluconazole (Diflucan) are reasonably potent. Garlic and probiotics supplements are natural antifungls. Treatment must include lowering of carbohydrate in diet and should include removal of chemicals as from carpeting and plywood sub-flooring.
If toxins from abnormally abundant Candida can inflict damage to enzyme production, and PST in particular, then this combination of anti-fungal medication, supplements and low-carbohydrate diet for combating yeasts offers promise of long-term resolution of ADHD.
For what it's worth, a far out note will be thrown in here. Could leaky blood-brain barrier allow chemicals to cause the ear ringing called tinnitus? A significant fraction of tinnitus cases are obviously due to loud-sound shock, such as with the Navy veterans who served on battleships. But this author has tinnitus in two forms, a fixed persistent level plus a variable component often random in timing but sometimes correlating with ingested or breathed chemicals.
The most noticeable variable incidents involved alcohol IV and gasoline vapor. There was very loud and sudden onset four to five seconds after administration of an IV saline flush containing 0.09% benzyl alcohol preservative.(Abbott Laboratories, NDC 0074-1966-07) The tinnitus sustained at fixed level, and subsequent saline flushes twice a day did not increase the perceived sound intensity. A whiff of gasoline fumes used to have similar effect, sudden onset of loud tinnitus. But in this case the exposures were far enough apart in time for the induced tinnitus to decay and for reexposure to cause repeat of the same sudden onset. This kind of pronounced effect occurring seconds after exposure has to be through the blood-brain barrier with no time for the liver to metabolize and circulate aldehyde.
A small amount of alcohol is produced as a byproduct of body metabolic process, about 3 ml/day, and ten seconds of that, 0.3 µl, is the same amount of alcohol as in the IV saline flush. Could the fixed persistent level of tinnitus be caused by metabolic waste products, or ingested chemicals, perhaps turned problematic by increased capillary permeability?
It might be interesting to see if other tinnitus patients respond to low doses of veinous alcohol or other chemicals and then to do differential before-after imagery. That would be more sensitive than the usual absolute readings. Cochlear nerves enter the brain stem at the superior olivary nuclei where right-left comparison circuitry aids determination of sound direction, are relayed to the inferior colliculus,(a,b)
and from there to the thalamus (I/O port) and then to the primary auditory cortex of the brain. The inferior colliculus may serve as a volume control center, and if veinous challenges worked, tinnitus onset timing could be controlled to a half second or so, and it would be interesting to look for response changes in inhibitory or excitatory neurotransmitters using the specific probes of PET. And is there any relationship between leaky blood-brain barrier, if it occurs, and leaky gut syndrome?
Shaw's Correlation of Yeast with Autism and Hyperactivity
ADHD and autistic children have usually been given considerable oral antibiotics early in life and often display a litany list of "Candida" symptoms in addition to their behavior and attention problems. A quantitative example is given by
Shaw, director of the laboratory that first applied mass spectrometry to urine analysis. He found non-human waste products in autistic and ADHD patients and showed that these waste products come from abnormal microorganisms in the gut - sometimes at near lethal dose.
Tartaric acid as opposed to normal malic acid turned out to be a particularly telling example. Tartaric acid is found at only low levels in the urine of normal patients (typically 15 mmol/mol of creatinine). It is not a human wast product but is produced instead by Saccharomyces cerevisiae or baker's yeast, which is abnormal if abundant in the gut. Tartaric acid interferes with normal human biochemistry of the very similar compound, malic acid, and whence with the Krebs cycle and the basic cellular-level supply of energy.
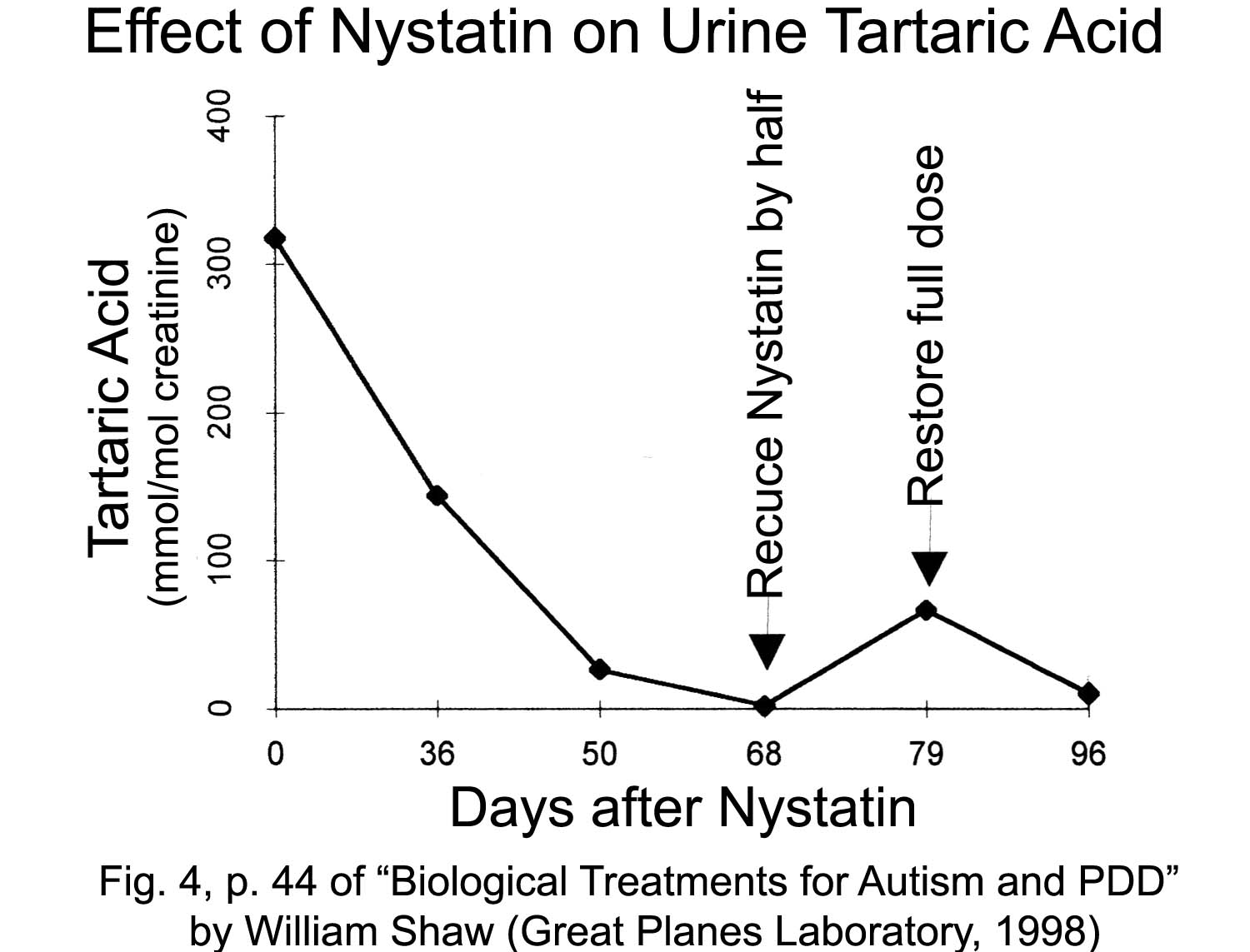 The plot on the right shows the amount of tartaric acid present in the urine of an autistic child who had already been started on Nystatin treatment several days before the first mass spectrometric urinalysis. Before treatment the child had lost most normal development and was extremely hyperactive. Eye contact was returning, the hyperactivity was abating, and the child slept through the night after a few days of Nystatin - which is when the urinalysis began - and improvement continued thereafter. The measured tartaric acid excretion was slowly dropping to normal levels during the administration of the anti-fungal medication, and this was in step with parent-reported improvement in the patients clinical symptoms. An initially striking surprise in the plot, though, was the rebound of tartaric acid when the dose level of Nystatin was temporarily reduced. The parents had halved the pills when they needed a refill and were about to run out of the medicine. Shaw concludes about the plot that once in ascendance, and perhaps even having modified the DNA of human intestinal cells, unfriendly microflora of the gut can be highly resilient.
The plot on the right shows the amount of tartaric acid present in the urine of an autistic child who had already been started on Nystatin treatment several days before the first mass spectrometric urinalysis. Before treatment the child had lost most normal development and was extremely hyperactive. Eye contact was returning, the hyperactivity was abating, and the child slept through the night after a few days of Nystatin - which is when the urinalysis began - and improvement continued thereafter. The measured tartaric acid excretion was slowly dropping to normal levels during the administration of the anti-fungal medication, and this was in step with parent-reported improvement in the patients clinical symptoms. An initially striking surprise in the plot, though, was the rebound of tartaric acid when the dose level of Nystatin was temporarily reduced. The parents had halved the pills when they needed a refill and were about to run out of the medicine. Shaw concludes about the plot that once in ascendance, and perhaps even having modified the DNA of human intestinal cells, unfriendly microflora of the gut can be highly resilient.
Chemical Imbalance Treatments a la Pfeiffer, Walsh, Rimland
Another non-pharmaceutical approach for the spectrum of conditions from ADHD to autism and violent behavior is testing and treatment for biochemical imbalances in metabolic pathways, often reflected in heavy metal anomalies. This was pursued initially by Pfeiffer for schizophrenia and then more generally and rigorously by Walsh (a, b) and others. And chelation therapy is part of Rimland's ARI treatments for autism. The focus of the present write up, though, is explanation of the Feingold community's view that artificial chemicals are often or usually the immediate cause of ADHD.
The Clinical Ecologists, 1940s-1970s
A wide range of physical and mental symptoms caused by foods and environmental chemicals was first correlated by Theron G. Randolph and other Clinical Ecologists of the 1940s. This extended through Mandell's publication in 1979, with one of his
case histories
heralding the then unknown link to Candida and ADHD. The Clinical Ecologists were essentially laughed out of town by mainstream medicine and directed not to do allergy testing in mental hospitals.
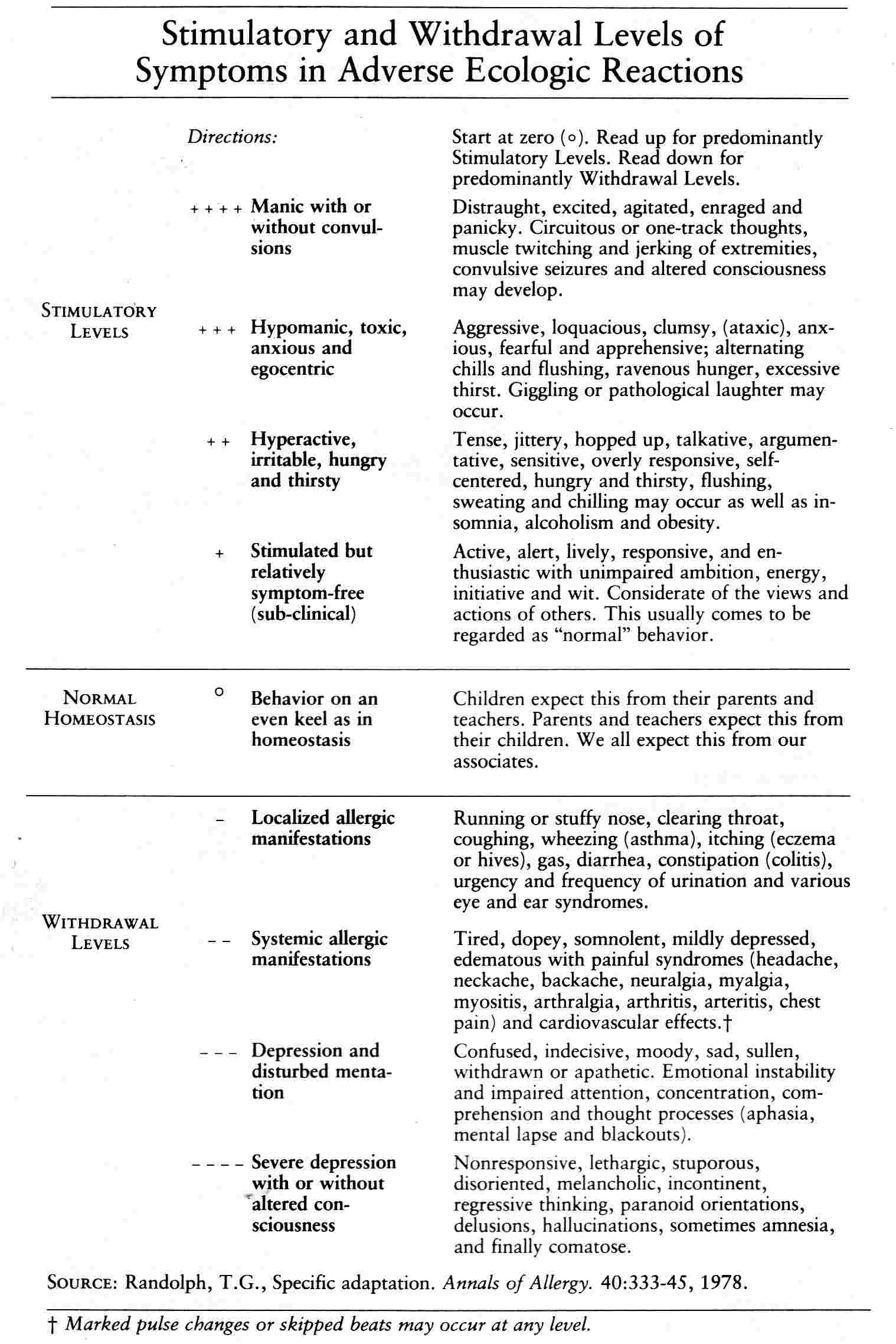
Still, there are perhaps three offshoots surviving from that era. 1) The body chemistry abnormalities evaluated by Walsh and others as described above are in a sense derived via Pfeiffer, who first correlated mental illness with heavy metal imbalance. 2) Truss's ideas about Candida seem, as described above, to provide an explanation for the diverse list of physical symptoms first described by the Clinical Ecologist. Anti-fungal medications like Nystatin and Dyflucan are used today, but the effectiveness of Mandell's fast appears to have been an early primitive way of combating fungi. (Truss seems not to have been aware of this earlier work by the Clinical Ecologists.) 3) It was Randolph, not Feingold, who first used diet to control hyperactivity. There were essentially no artificial chemicals being added to foods in the 1940s, and there was no ADHD epidemic then, but as listed in the table below, hyperactivity reactions and worse were sometimes being observed as reactions to foods and environmental chemicals. The list is broad (too broad for some to believe), and in part encompasses what today might be called ADHD and comorbid conditions.
A provocative point suggested by Mandell was that, if problem foods can affect the central nervous system and behavior, they might also be expected to affect the autonomic parasympathetic system as well, making them likely candidates for causing conditions like high blood pressure and "Type A" personality for heart problems. This is not in Mandell's table, is not mentioned by proponents of the Feingold Program and indubitably is not part of mainstream's list of conditions comorbid with ADHD.
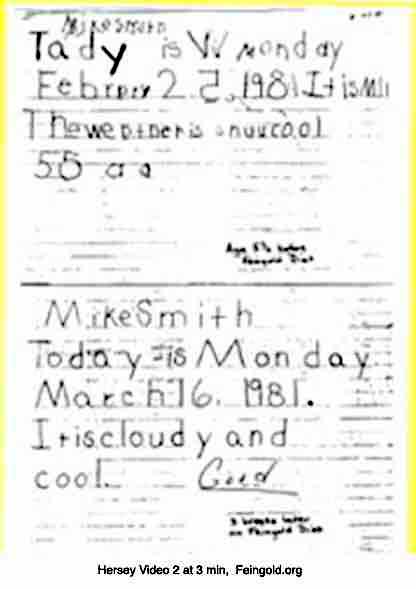
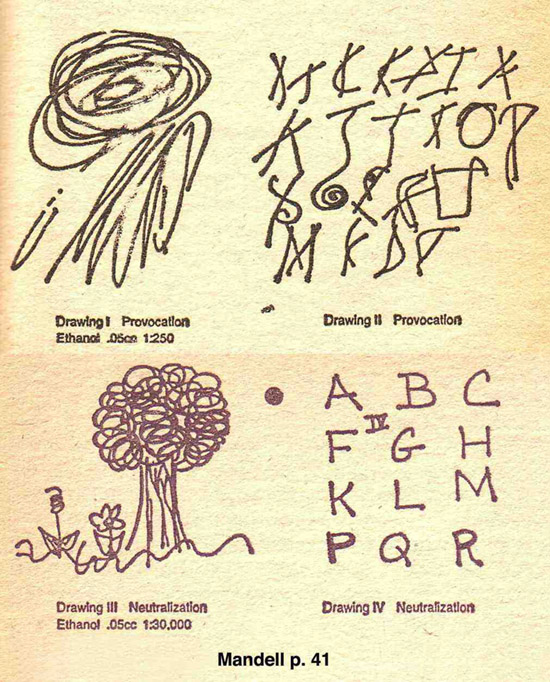 Threshold allergy testing and desensitization dose level are perhaps the most resisted findings of the Clinical Ecologists. These are used today by only a few holistic doctors and ENT specialists apparently careful not to call themselves Clinical Ecologists, but still sometimes referred to by mainstream as "an embarrassment to the profession with patients who should be seeing a psychiatrist, not an MD."(Personal conversations with Dr. Richard Feinburg) A problem is that the reactions do not always occur and so can be used only as indicators rather than as reliable allergy tests. But they do occur. The first figure on the right is from Mandell's book and shows what might be called variable dyslexia.(click to enlarge) The scribble writing and drawing is in response to 0.05 cc of 1:250 subdermal ethanol. The normal writing and drawing was by the same patient only a few minutes later after a 100 times weaker desensitization dose. The second figure is from FAUS, the dyslexic writing by an ADHD child correcting after a few weeks of the Feingold Program.
Threshold allergy testing and desensitization dose level are perhaps the most resisted findings of the Clinical Ecologists. These are used today by only a few holistic doctors and ENT specialists apparently careful not to call themselves Clinical Ecologists, but still sometimes referred to by mainstream as "an embarrassment to the profession with patients who should be seeing a psychiatrist, not an MD."(Personal conversations with Dr. Richard Feinburg) A problem is that the reactions do not always occur and so can be used only as indicators rather than as reliable allergy tests. But they do occur. The first figure on the right is from Mandell's book and shows what might be called variable dyslexia.(click to enlarge) The scribble writing and drawing is in response to 0.05 cc of 1:250 subdermal ethanol. The normal writing and drawing was by the same patient only a few minutes later after a 100 times weaker desensitization dose. The second figure is from FAUS, the dyslexic writing by an ADHD child correcting after a few weeks of the Feingold Program.
One preservative that was in use in the 1940's is the gas used to preserve prunes. Randolph found this to be the laxative agent rather than the fruit itself. But it was not until after world war II that artificial colorings, flavorings and preservatives began to be added to foods, and by 1970 Feingold was noting an increase in hyperactivity responses specifically to these chemicals. Interestingly, Feingold did know Randolph, according to a Feingold protege, so it looks perhaps a little unprofessional for him not to have referenced the overlapping works that preceded his own. There is a very big difference is the path they took. Randolph was strictly clinical, listening carefully to patients. Feingold followed a logic path. find money for allergy research for the ubiquitous Bay area flea, the flea bite allergy is to a small chemical called a hapten too small to trigger the immune system, the reaction is due to union of a small insect saliva hapten with a large human collagen skin molecule, drug molecules are small, too, so look for drug allergies, reactions to aspirin were found, and then to salicylate, and then discovery of how aspirin works pointed to prostaglandins and the idea that reactions could be provoked by compounds with no structural relationship to the triggering chemical, whence investigation of artificial colorings and flavorings. But, still, there is an overlap in the end results that they found, and the Clinical Ecologists were first, so Feingold should probably have acknowledged them. Clinical Ecologist Mandell's 1979 book cites Feingold.
Now in the years since Feingold, FAUS has significantly refined and perfected the diet regimen for alleviating ADHD, and both that organization and some researchers have found that common foods can sometimes be causal as well as the now ubiquitous and plentiful chemical additives. That can be viewed as essentially a rediscovery of the below table except modified to emphasize the causality of modern food chemicals, the "Feingold diet" then being a follow on from the Clinical Ecologists of the 1940s. The most recent rediscovery is at WhyDye.org.
Clinical Ecology:
- Human Ecology and Susceptibility to the Chemical Environment,* by Theron G. Randolph, (Charles Thomas, 1962)
- An Alternative Approach to Allergies, by Theron G. Randolph and Ralph W Moss, (Bantam Books, 1980)
- Clinical Ecology, A New Medical Approach to Environmental Illness, by Iris R Bell, (Commonweal Research, 1982)
- 5-Day Allergy Relief System, by Marshall Mandell and Lynne Scanlon, (Pocket Books, 1979)
Candida albicans early texts:
- Missing Diagnosis, by C. Orion Truss, (1985, a collection of journal publications from 1980)
- Candida, A Twentieth Century Disease, by Shirley S. Lorenzani, (Pivot Original Health Books, Keats Pub Inc, 1986)
- The Yeat Syndrome, by John Parks Trowbridge and Morton Walker, (Bantam, 1986)
*Written for medical professionals using terminology difficult for the average reader.
PSD Deficiency Model
The simplest summary of all the above for explaining causes of ADHD is that:
a) antibiotics and high carbohydrate diets may induce abnormal abundance of intestinal fungi,
b) the toxins from which might cause enzyme deficiencies including,
1) insufficient PST, exacerbated by ingestion of phenolic compounds in food additives,
2) which in the brain might be compensated for by increased production of MAO,
4) this causing mental suppression including processing and control parts of the brain, and so
5) attention deficit and poor judgement control of impulses from the emotional part of the brain,
6) this then making several of the food additives causal to ADHD with comorbid conditions,
7) but in trace amounts and detail that are inconceivable to many.
(This PST deficiency model has not been confirmed, and is somewhat incomplete and inconsistent in principle as pointed out above.)
(Precursors a & b come from the separately disputed concept of whether Candida overgrowth could cause systemic dysfunctions.)
(They suggest, though, that an anti-Candida diet may offer long-term resolution of ADHD, the restricted diet good for short-term.)
Conclusions
TBD
1) FDA Food Advisory Meeting - for Tartrazine:
It might be advisable for the FDA to host another Food Advisory Committee for evaluation of food coloring. But this time don't try anything not allowed by law, and don't use people inexperienced with the subject diet. Specifically:
Evaluate tartrazine, (Yellow #5), for whether there is sufficient evidence for requiring warning labeling or for banning use. There is unique compound-specific challenge testing for tartrazine as required by law.
Committee members and the FDA staff should be familiar with what the Feingold diet has evolved to today. They should at least having read the defining materials from FAUS, and a good fraction of Committee and staff should have personal experience having used these aids and having seen the Feingold diet work with their own ADHD child. If this significant fraction can not be drawn from government employees, the slots should be filled with qualified contractors.
Committee members should have read Rowe1994 and Levy1978a and be familiar with the differences in protocol.
One of the Rowe's should be invited to present plus someone with opposing findings as an author of AACAP1997 or Levy1978a.
2) …
Updates
Most needed are: a technical revision of the analysis of the key dozen journal papers. Most of this web site was written before 2012 with the initial 19 paragraphs revised in 2020.


){kind=link}